
Jaw Pain: Temporomandibular Joint Disorder Treatment

“TMD is reported in 20-30% of the population.”
Did you know that the temporomandibular (jaw) joints are one of the most frequently used joint in the body, as they need to open and close to 2000 times per day (talking, chewing, breathing, swallowing, and yawning). This means they move a lot during the day, but yet they likely receive the least amount of attention during physiotherapy treatment. When it comes to understanding the jaw, it can be intimidating to understand all the structures and joints involved. We are here to break it down into bite size pieces.
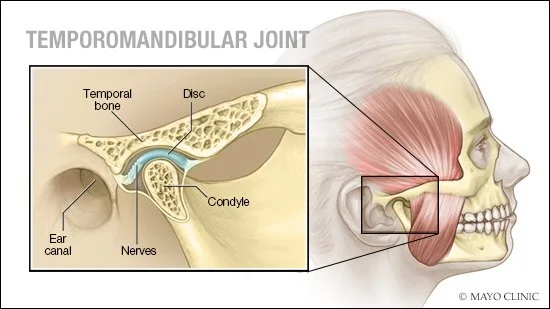
The temporomandibular joints (TMJ), also known as the jaw, is the anatomical structure located on either side of your face where your jaw hinges open and closed. This joint, like other joints in the body, can develop issues and disorders that prevent it from performing optimally and causes symptoms such as jaw pain, headaches, locking, and pain while chewing. Anatomical disorders that affect he TMJ are known as Temporomandibular Joint Disorder (TMD). TMD also includes disorder of the masticatory muscles (muscles in the face that move the jaw), and other associated structures of the TMJ (Selvam & Ramachandran, 2017).
TMD is a major public health problem as it is the main source of chronic orofacial pain and the most prevalent category of non-dental chronic pain conditions in the orofacial region (Calixtre, Oliveira, Alburquerque-Sendin & Armijo-Olivo, 2020). The severity of TMD can range from mild to severe, and the symptoms include:
Pain
Restricted jaw movement
Headaches
Clicking/popping
Locking
Tinnitus
Grinding
Clenching
Feeling of fluid in your ears
Why does it occur?
It’s etiology (cause) is multifactorial and multidimensional, it involves neurobiological, biomechanical, neuromuscular, and biopsychological factors (Calixtre, Oliveira, Alburquerque-Sendin & Armijo-Olivo, 2020). Due to this we take a multidimensional treatment approach and ensure that we offer explanations of why symptoms likely occur.
What is all this ringing about?
Tinnitus is the term for hearing sounds in the inner ear that are not from an external source (can be mild to severe. The anatomical relationship between the TMJ and the ear begins with early embryonic development. Due to the proximity of the cranial nerves to the TMJ hyperactivity of these nerves can cause tinnitus. The interaction between tinnitus and TMD is a complex issue, but it is known to be more prevalent among those suffering from TMD when compared to the general population. Conservative treatment such as physiotherapy is shown to provide significant improvements (Feitoza & Menezes, 2018).
How is TMD treated?
Due to evidence and our clinical experience, we utilize a multidimensional treatment plan. This involves education of your condition, manual therapy, home exercises, self-management techniques, acupuncture, and dry needling. We follow up with you to consistently modify and progress your program, so you achieve your goals. We also work with several TMD medical specialists, dentists, orthodontist, and we will regularly communicate with them to form a collaborative team. Learn more about TMD treatment below:
Education
We educate you about TMD and the associated symptoms, so that you can better understand your treatment plan.
Manual Therapy + Exercise: Supported through clinical experience and research
Manual therapy in physiotherapy is characterized by fine manipulative techniques, which are less invasive than others. It is utilized to improve joint range of motion, manage myofascial tone, and to restore the circulation of body fluids (Selvam & Ramachandran, 2017). It is also utilized to correct aberrant motor behaviors, enhances tissue extensibility, and helps with relaxation (Asquini, Rushton, Pitance, Heneghan, Falla, 2021).
Acupuncture/Dry Needling
Like all our treatment approaches, this is supported through evidence. This treatment intervention is shown to reduce symptoms associated with TMD.
Dry needling is a procedure where a fine needle is inserted into the skin and muscle to target myofascial target points. These are hyperirritable spots in the skeletal muscle that have a palpable nodule, which can cause weakness, restricted ROM and local or referred pain (Physiopedia, 2021). Acupuncture is the use of needles that pierce the skin at the acupuncture points. The physiotherapist determines the location of these points based on their assessment and the cause of the imbalance. A number of needles may be used during treatment, and are typically left in position for around 20 minutes before being removed (Physiopedia, 2021).
Outcome Measures That We Utilize:
Outcome measures look at how a particular condition is affecting your daily activities, pain levels, or function. These are filled out with your physiotherapist to give you a baseline understanding of your condition and symptoms, and then later reassessed to determine what symptoms are improving from treatment. These measures include:
Headache Impact Test (HIT-6)
Mandibular Function Impairment Questionnaire (MFIQ)
Maximum Mouth Opening
References
Selvam, P. S., & Ramachandran, R. S. (2017). A Comparative Study on the Effectiveness of Manipulative Technique and Conservative Physiotherapy Modalities in Correction of Temporo-mandibular Joint Disorder. Indian Journal of Physiotherapy & Occupational Therapy, 11(3), 195–200. https://doi-org.login.ezproxy.library.ualberta.ca/10.5958/0973-5674.2017.00103.4
Cavalcante Feitoza, C., & de Lemos Menezes, P. (2018). Prognosis of conservative treatment in individuals with temporomandibular disorders and tinnitus: a systematic review. Muscles, Ligaments & Tendons Journal (MLTJ), 8(1), 123–134.
Calixtre, L. B., Oliveira, A. B., Alburquerque-Sendín, F., & Armijo-Olivo, S. (2020). What is the minimal important difference of pain intensity, mandibular function, and headache impact in patients with temporomandibular disorders? Clinical significance analysis of a randomized controlled trial. Musculoskeletal Science & Practice, 46, 102108. https://doi-org.login.ezproxy.library.ualberta.ca/10.1016/j.msksp.2020.102108
Cavalcante Feitoza, C., & de Lemos Menezes, P. (2018). Prognosis of conservative treatment in individuals with temporomandibular disorders and tinnitus: a systematic review. Muscles, Ligaments & Tendons Journal (MLTJ), 8(1), 123–134.
Asquini, G., Rushton, A., Pitance, L., Heneghan, N., & Falla, D. (2021). The effectiveness of manual therapy applied to craniomandibular structures in the treatment of temporomandibular disorders: protocol for a systematic review. Systematic Reviews, 10(1), 70. https://doi-org.login.ezproxy.library.ualberta.ca/10.1186/s13643-021-01623-7
Touche, R. L., García, S. M., García, B. S., Acosta, A. P., Juárez, D. A., Pérez, J. J. F., Angulo-Díaz-Parreño, S., Cuenca-Martínez, F., Paris-Alemany, A., & Suso-Martí, L. (2020). Effect of Manual Therapy and Therapeutic Exercise Applied to the Cervical Region on Pain and Pressure Pain Sensitivity in Patients with Temporomandibular Disorders: A Systematic Review and Meta-analysis. Pain Medicine, 21(10), 2373–2384.
Cho, S.-H., & Whang, W.-W. (2010). Acupuncture for temporomandibular disorders: a systematic review. Journal of Orofacial Pain, 24(2), 152–162.